
Consistent with the guideline recommendations, the committee adapted the HEARTS framework to develop suggested algorithms for the diagnosis (Figure 2) and treatment ( Figure 3) of hypertension in the Canadian primary care setting.8 Standardized protocols are effective in improving population-wide BP control. A recent meta-analysis of RCTs demonstrated that standardized treatment protocols reduce mean systolic and diastolic BP by 6.7 (95% CI 3.7–9.8) mm Hg and 2.6 (95% CI 1.2–4.1) mm Hg, respectively, compared with usual care.101With broad adoption, specific algorithms can reduce drug costs through bulk drug purchasing and make standardized education and task-sharing more efficient and less costly.11

Implementation
Figure 2:
Suggested algorithm for the diagnosis of hypertension in primary care. Note: ABPM = ambulatory blood pressure monitor, BP = blood pressure, HBPM = home blood pressure monitor. *Continue yearly or opportunistic BP monitoring. Perform out-of-office BP assessment if masked hypertension is suspected. †If unavailable or infeasible, repeat office BP assessment at a separate visit. ‡Use Hypertension Canada–recommended or other validated home BP devices. §Continue yearly or opportunistic BP monitoring.
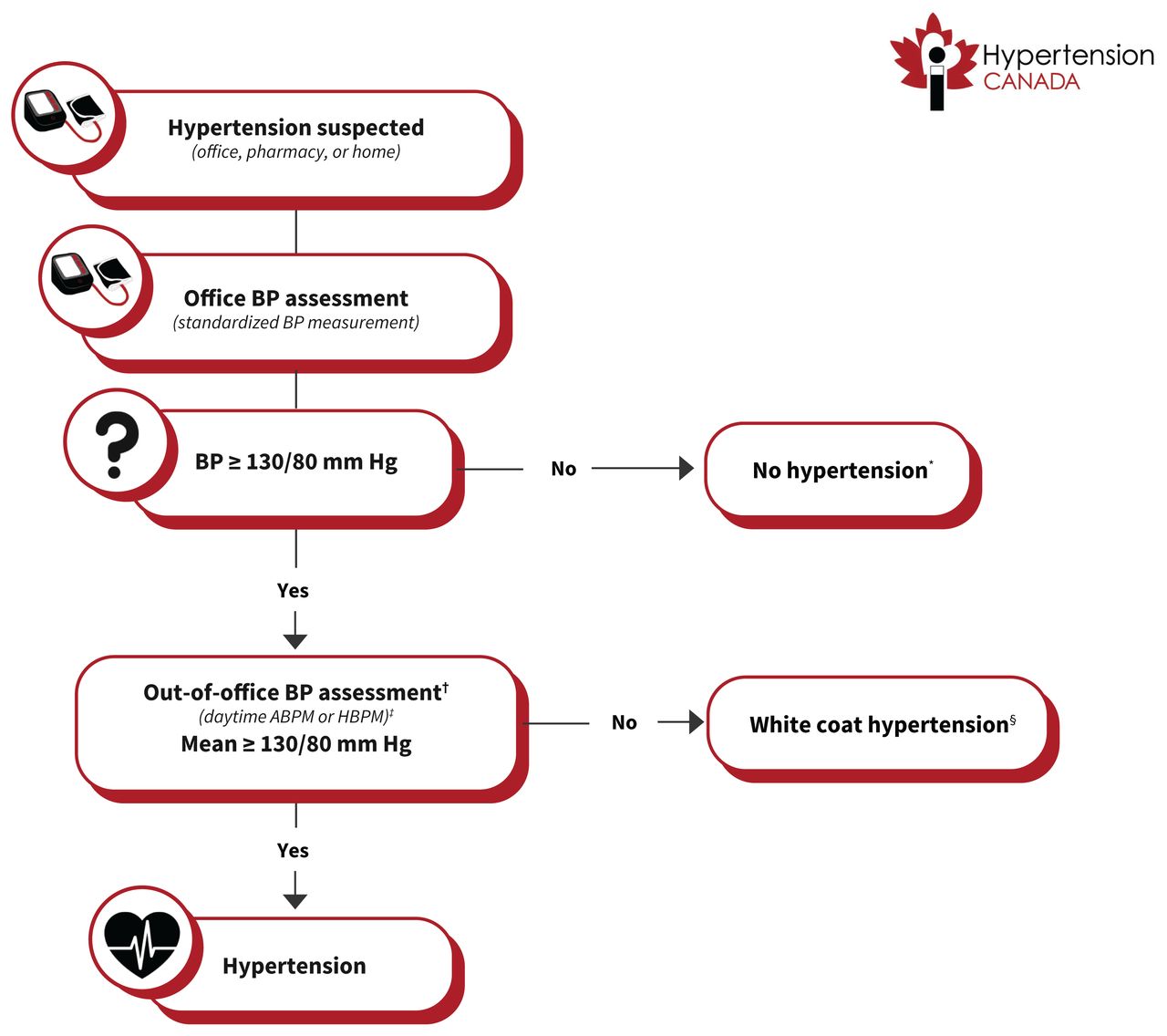
Figure 3:
Suggested algorithm for the treatment of hypertension in primary care (not intended for use in pregnancy). Note: BP = blood pressure, CVD = cardiovascular disease, eGFR = estimated glomerular filtration rate, HCTZ = hydrochlorothiazide, SBP = systolic blood pressure. *High CVD risk conditions include established CVD (coronary artery disease, heart failure, cerebrovascular disease, and peripheral artery disease), type 1 or type 2 diabetes mellitus, chronic kidney disease (eGFR < 60 mL/min/1.73 m2 or albuminuria ≥ 3 mg/mmol), 10-year Framingham Risk Score ≥ 20%,62 and age ≥ 75 years. †Initial single-pill combination therapy is preferred if available and covered. If not, 2 separate pills can use used as an alternative, with preference for a long-acting thiazide-like diuretic over a thiazide diuretic. If patient is at high risk of symptomatic hypotension, treatment initiation with a single agent is reasonable. Angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers should be avoided or discontinued in all people who are pregnant or trying to become pregnant. ‡See Table 3 for acceptable alternative single-pill combinations available in Canada. §Includes unexplained, sudden worsening of hypertension, hypokalemia, adrenal nodule, abdominal bruit, acute kidney injury after hypertension treatment, severe or malignant hypertension, hypertension at a young age, and resistant hypertension.
Factors we considered for the recommended drug selection within the algorithm included efficacy, tolerability, cost, coverage, availability, protection from future drug shortages, and ability to split pills (Appendix 2). Based on these, we selected a combination pill with irbesartan and hydrochlorothiazide as the preferred initial combination therapy at this time, although the initial combination will be periodically reconsidered given availability and new evidence to suggest more cost-effective choices. Acceptable alternative single-pill combination therapies currently available in Canada are listed in Table 3.
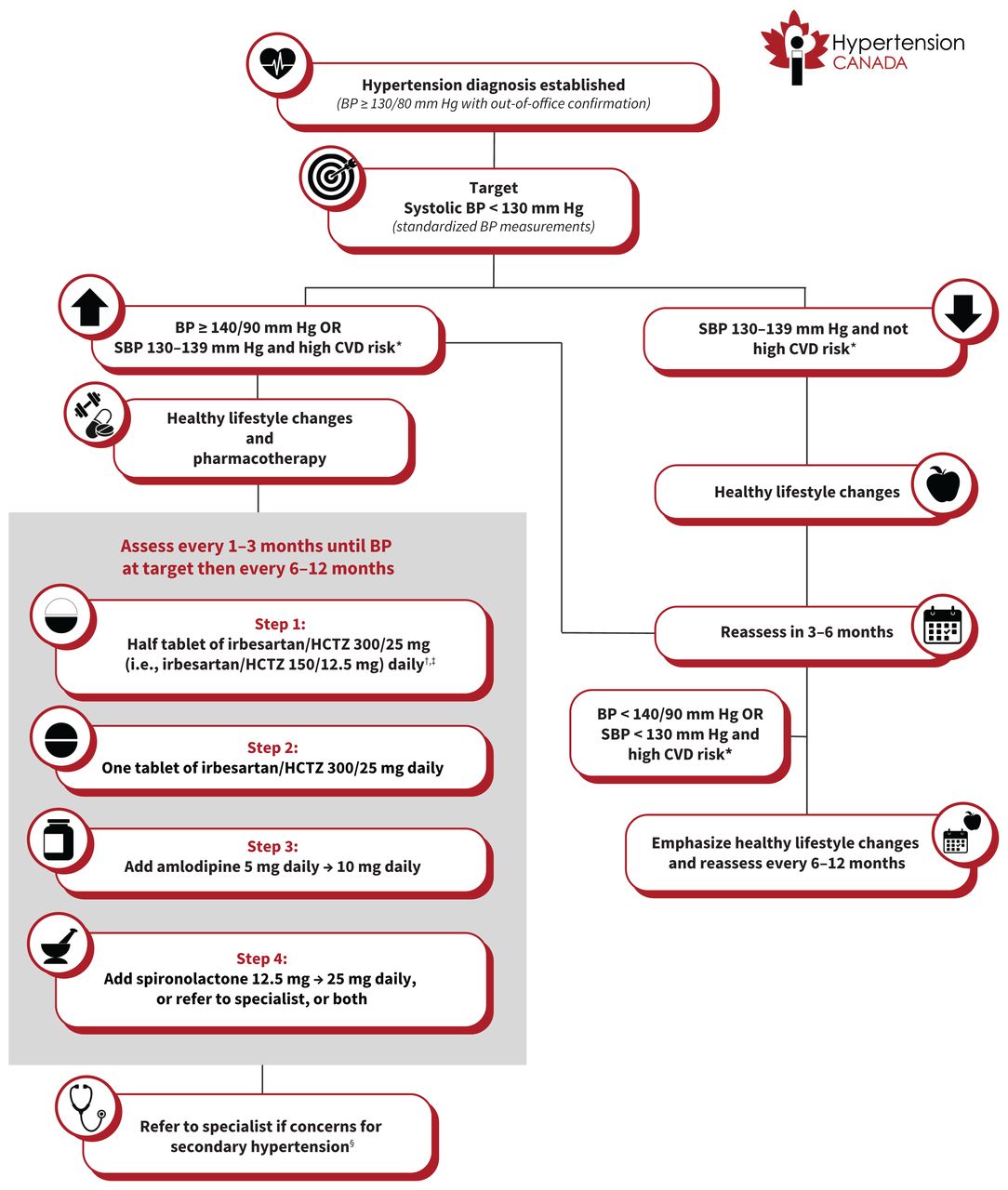
Table 3:
| Single-pill combinations | Cost for 30 days of combination pills, $Can* | Cost for 30 days of the individual drug equivalents, $Can* |
|---|---|---|
| ARB + thiazide or thiazide-like diuretic | ||
| Irbesartan–hydrochlorothiazide | 6.55 | 7.31 |
| Telmisartan–hydrochlorothiazide | 6.29 | 6.95 |
| Olmesartan–hydrochlorothiazide | 8.12 | 8.76 |
| Candesartan–hydrochlorothiazide | 7.33 | 7.25 |
| ACEI + thiazide or thiazide-like diuretic | ||
| Lisinopril–hydrochlorothiazide | 7.51 | 6.31 |
| Perindopril–indapamide | 8.58 | 12.04 |
| ARB + long-acting dihydropyridine CCB | ||
| Telmisartan–amlodipine | 16.42 | 12.47 |
-
Note: ACEI = angiotensin-converting enzyme inhibitor, ARB = angiotensin II receptor blocker, CCB = calcium channel blocker.
-
↵* Drug costs obtained from https://www.ramq.gouv.qc.ca/fr, https://www.formulary.health.gov.on.ca/formulary/, and https://pharmacareformularysearch.gov.bc.ca/ (accessed 2025 Feb. 5).
Available single-pill antihypertensive medication combinations in Canada and associated costs
Importantly, the cost of most single-pill combinations is generally lower than the cost for the equivalent individual components. It should be noted that the lower BP thresholds adopted for both defining hypertension and treatment targets relative to previous Hypertension Canada guidelines means that a higher number of people will be labelled as having hypertension, which may have meaningful personal implications (e.g., stigma, insurance). 31 However, the committee thought that the contemporary evidence strongly supports the lower thresholds to promote early detection of, and intervention for, hypertension, which will translate into mitigating long-term cardiovascular complications at the population level.
The HEARTS framework has a well-established implementation policy to engage primary care and optimize guideline uptake, which will be leveraged for this purpose within Canada.8 This includes active engagement with primary care centres, along with the development of knowledge transfer tools to support health care providers and patients. These tools include a downloadable patient support tool, to be made widely available for posting in clinics and provision to patients as educational handouts (Appendix 4, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.241770/tab-related-content). Additional free online resources for health care providers and patients are listed in Appendix 5, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.241770/tab-related-content.
Timely dissemination of the guideline content and implementation tools will take place via the Hypertension Canada website (https://hypertension.ca) and network, social media, podcasts, and national primary care conferences. Successful implementation will be tracked via downloads of the patient support tool, traffic to the guideline website, and prospective trends on hypertension treatment and control rates, which Hypertension Canada has traditionally captured via the Canadian Health Measures Survey.5
Hypertension Canada will update this guideline when new data pertinent to the diagnosis and treatment of hypertension emerge or when new cost-effective antihypertensive combination pills become available in Canada.